The
increasing prevalence of diabetes reinforces the need for improved management
of its complications. Diabetic retinopathy (DR) represents one of the most
significant complications of diabetes, being one of the leading causes of
blindness in the world [3]. Diabetes is defined by hyperglycemia and is
becoming more prevalent. Diabetic retinopathy occurs when blood vessels in the
retina leak leading to damage and disruption of vision [20]. Research shows
that about 40% to 45% of patients with diabetes will have DR in their lifetime.
Predictions made by the International Diabetes Federation (IDF) indicate a
sharp rise in the number of people who will have diabetes, expecting to go from
537 million today to 643 million by 2030[4]. In India, the situation is dire;
the Indian Council of Medical Research estimates that there are more than 10
million people living with diabetes [21]. Numbers of this magnitude supports
the need for improved management of complications related to diabetes with the
largest representation of these complications being found with DR [19].
At
present, diagnosing and grading DR entails that a health care provider on the
patient's behalf, requires that an eye doctor or specialist performs a manual
examination. It can be a very long process and can be subjective in nature,
resulting in inconsistency of results[8][22]. For that reason, it is necessary
to develop better systems for accurate and quick detection and grading of diabetic
retinopathy. Automated systems are emerging using deep learning and have been
shown to effectively classify retinal images allowing for valuable deep
learning based systems to effectively and accurately assess retinal images for
the presence of DR lesions[5].
This research aims to advance the
field by introducing a new automated DR grading methodology based on ensemble
deep capsule networks. By taking advantage of pre-trained CNNs and ensemble
learning models and capsule networks, this new module aims to improve DR
diagnosis performance by providing enhanced robustness based on the trained
models[7][25]. The input for our automated system will be fundus images, which
will subsequently classify the different stages ranging from diabetes without
diabetic retinopathy (NoDR), mild non-proliferative DR (NPDR), moderate NPDR,
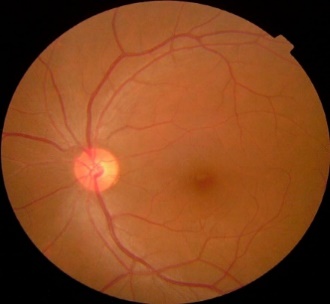
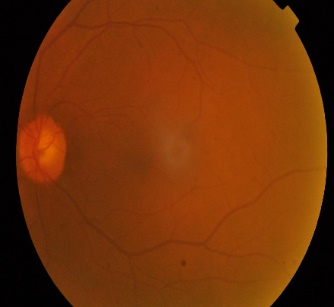
severe NPDR, and proliferative DR (PDR) [1][2]. Figure 1 shows the categories
and the classification differences based on fundus images. Deep learning has
recently revolutionized automated detection of DR from retinal fundus images,
lessening the reliance on expert ophthalmologist specialists, and the necessary
initial screening steps[23][24]. Overall, deep CNNs have shown great
performance in extracting discriminative features in an effort to classify DR
and other base line disease stages, but they have also generally failed to
account for spatial features and relationships among features in pooling
layers, as well as structures of faint lesions needed to grade severity of DR. Capsule
networks (CapsNets), developed by Sabour et al., eliminate this limitation by
preserving part-whole relationships with dynamic routing algorithms, thereby
encoding spatial hierarchies in medical images in an advanced way [26].
Nonetheless, when using capsule networks with large-scale fundus datasets, two
major issues arise: high computational costs which limit scalability and
performance saturation, in which accuracy eventually reaches a plateau and does
not improve as model complexity increases [6].
|
|
|
|
|
(a) No DR
|
(b) Mild NPDR
|
(c) Moderate NPDR
|
|
|

|
|
(d) Severe NPDR
|
(e) PDR
|
Figure 1. Samples of different stages of DR.
Despite encouraging results from both CNNs
and capsule networks, existing DR grading approaches are constrained by three major
limitations: single-stream architectures that fail to leverage complementary
feature representations from different network families, deterministic fusion
strategies that can overfit to dataset-specific characteristics and reduce
generalization, and insufficient ablation studies that leave the relative
contribution of individual architectural components poorly understood[21][35].
To
address these gaps, this study proposes a Stochastic Ensemble Dual-Stream
Capsule Network for multi-class DR grading. The framework incorporates several
key innovations:
•
A
dual-stream architecture that integrates ResNetV2 and MobileNet backbones in
parallel, enabling simultaneous extraction of complementary global and
lightweight features.
•
Capsule-based
feature preservation, where capsule layers retain spatial relationships
critical for accurate lesion localization and DR severity discrimination.
•
A stochastic
ensemble fusion mechanism, in which randomized weighting during feature fusion
mitigates overfitting and enhances robustness to domain shifts.
•
A
comprehensive evaluation pipeline that includes extensive experiments on the
APTOS 2019 dataset, ablation studies, hyperparameter tuning, and
state-of-the-art comparisons, demonstrating substantial performance
improvements.
The
remainder of this paper is organized as follows: Section 2 reviews related work
in DR detection using CNNs, capsule networks, and hybrid architectures. Section
3 describes the proposed methodology in detail. Section 4 presents experimental
results, ablation analyses, and comparative evaluations. Section 5 concludes
the study and outlines potential directions for future research. Furthermore,
our methodology advances scientific visualization by providing clearer
class-specific representations of DR stages through capsule-based spatial
feature mapping. By visualizing feature hierarchies and lesion-sensitive
regions within fundus images, our framework contributes to the emerging field
of visual analytics in medical AI.
Diabetic retinopathy (DR) is a serious
health concern impacting individuals worldwide and has spurred numerous
research efforts aimed at improving diagnosis and treatment. Convolutional Neural
Networks (CNNs) have emerged as effective methods for automatically grading DR
due to their ability to analyze fine details in retinal images. Numerous
researchers have attempted different design features and approaches for CNNs to
enhance the accuracy and efficiency of DR classifications.
To mitigate the issue of over fitting in
CNNs, Tymchenko, Marchenko, and Spodarets employed data augmentation
techniques. In this case, they did not start from scratch by conducting
training on a CNN encoder as it was pre-trained. They also implemented a novel
approach of using three decoders: EfficientNet-B4, EfficientNet-B5, and
SE-ResNeXt50 to classify diabetic retinopathy (DR) lesions. The final
prediction was made by feeding a linear regression model into the outputs. When
combining the results sourced from three models and utilizing a dataset from Aptos
(Aptos-19-5829 dataset, Yang et al., 2019), the authors obtained a DR detection
accuracy of 99.3%. To achieve greater classification efficiency, various
researchers have focused on preprocessing methodologies such as image resizing
from the Aptos 2019 blindness dataset to a common reference format to support
learning efficiency. Gangwar and Ravi (2021) also enhanced their dataset in
order to tighten their models performance. With a hybrid model that included
custom CNN layers and Inception-ResNet-v2, their achieved quasi-accurate of
82.18%.
Equally,
another study employed an ensemble with three Efficient-Net models on an
augmented dataset, achieving a remarkable quadratic kappa score of 0.924377 on
the APTOS test dataset [9]. This indicates that ensemble learning can achieve
better model performance and reliability. In conclusion, both studies made
major advances in detecting diabetic retinopathy using deep learning and
additional application research must be conducted to determine how
transferrable these results would be in other datasets and clinical settings.In
a previous study conducted by Mishra, Hanchate, and Saquib [10], after
preprocessing steps performed on diabetic retinopathy (DR) images led to a
series of steps to crop, resize, and cleaned the fishing image. They
subsequently applied two CNN models, DenseNet-121, and VGG-16, respectively
using transfer learning especially around DenseNet-121, which showed greater
cautiously higher criteria than VGG-16 with this results using transfer
learning showed accuracy of 96.11% from a pre-trained DenseNet using IMAGENET,
and 73.26% for VGG-16 using data from the aptos-19 database. This points to the
significance of learning about CNN methods and learning around transfer
learning to be able to apply classification for DR. Mushtaq and Siddiqui [11]
also employed preprocessing steps like background and black corner removal and
scaling and applied Gaussian blur to the fishing images, as well as augmenting
their dataset with techniques to balance the dataset. Their application of
regression and DenseNet-169 models lead to results that yielded a reasonable
accuracy of 90% for DR classification, demonstrating the significant impact
that detailed pre-processing and dataset augmentation can have on model
performance and accuracy. In another methodology, AbdelMaksoud, Barakat, and
Elmogy [12] utilized an approach that involved resizing, cropping and
normalized the retinal images prior to DR classification. They also
incorporated a hybrid model as a classification mechanism, which included a
fine-tuned DenseNet BC-121 architecture block-Dense, Eyenet and three
convolution layers, and classified the DR into five classes accurately. This
leads us to believe that hybrid models may be capable of effectively capturing
different features, resulting in a better degree of accuracy for a multi-class
DR grading assignment. Lastly, Chowdhury et al. [13] created a preprocessing
pipeline that consisted of cropping, background removal and resizing, and when
they performed data augmentation to minimize their dataset's unbalance, they
performed a 5-fold cross-validation, and a 2-phase training method to reach
different learned weights with their model features generated using
EfficientNet-B5 extractor. In the end, their final ensemble model was able to
achieve a combined quadratic weighted kappa score of 0.96, which proved the
efficacy of their approach in a meaningful enough manner to produce
sufficiently performant DR detection models.
In general, the
studies reviewed show that deep learning methods are an effective approach to
automating the detection of diabetic retinopathy. These studies successfully
developed CNN models with more efficient preprocessing and improved
classification accuracy rates for diabetic retinopathy severity level
classifications. The studies pursued transfer learning, ensemble learning, and
hybrid models to increase classification performance and robustness across a
range of datasets. Despite the reported findings, the studies revealed
challenges in relation to issues such as dataset imbalance, model
interpretability, and generalizability to clinical use in real-world settings
enough to warrant future research studies. Overall, the reviewed studies
reported impressive accuracies, however to become applicable and reliable for
use in clinical practice is to validate accuracy against larger and more
diverse datasets. Summary of related works is shown in table 1.
Table 1
Summary of
Related works
|
Study
|
Method
|
Dataset
|
Performance
|
|
Tymchenko et
al. [7]
|
Ensemble:
EfficientNet-B4, B5, SE-ResNeXt50 + Linear Regression
|
APTOS 2019
|
Accuracy:
99.3%
|
|
Gangwar &
Ravi [8]
|
CNN +
Inception ResNet-V2
|
APTOS 2019
|
Accuracy:
82.18%
|
|
Karki &
Kulkarni [9]
|
Ensemble of
three EfficientNet variants
|
APTOS 2019
|
Quadratic
Kappa: 0.924
|
|
Mishra et al.
[10]
|
DenseNet-121
vs. VGG-16
|
APTOS 2019
|
DenseNet:
96.11%, VGG-16: 73.26%
|
|
Mushtaq &
Siddiqui [11]
|
DenseNet-169
|
APTOS 2019
|
Accuracy-90%
|
|
AbdelMaksoud
et al. [12]
|
DenseNet-BC121
+ Eyenet + CNN fusion
|
APTOS 2019
|
Accuracy-91.2%
Sensitivity-96%
Specificity-69%
DSC-92.45%
QKS-0.883
|
|
Chowdhury et
al. [13]
|
EfficientNet-B5
with a two-phase ensemble learning
|
APTOS 2019
|
Quadratic
Weighted Kappa score -0.961
|
The main aim of
this study is to create a sophisticated architecture that can efficiently
classify fundus images into five classes: no DR, mild NPDR, moderate NPDR,
severe NPDR, and PDR. Our objective will be reached by using an ensemble of
deep learning capsule networks and pre-trained deep learning CNN models that
will guarantee universal and constant performance in the study by appropriately
utilizing capsule networks' advantages for spatial representation and feature
extraction from various pre-trained CNN models.
This
research investigation experimented with different deep transfer learning
methods utilized in the APTOS 2019 blindness recognition dataset [37]. The 3662 images in the dataset
are divided into 5 classes, which are as follows: Figure 3 shows an example
from each category, while The entire amount of images in each classification is
displayed in Table 2. The classes are categorized by the dataset in this way:
No_DR is represented by Class 0, Moderate is characterized by Class 2, Severe
is characterized by Class 3, and PDR is characterized by Class 4.
Table 2: Amount of images for each class in the APTOS 2019 dataset
|
Class
Number
|
0
|
1
|
2
|
3
|
4
|
|
Number
of Images
|
1805
|
370
|
999
|
193
|
295
|
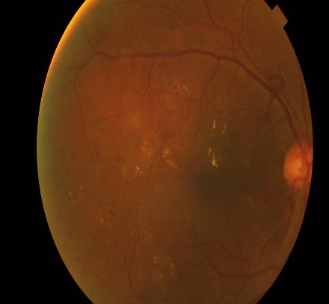
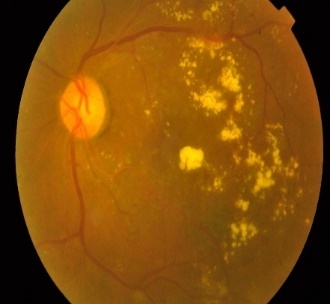
We used the
aptos-19 dataset for our experimental setup that contained images of varying
sizes. To maintain consistency and ease analysis, we resized all the samples
and recorded them in 256x256 pixels. We then pre-processed the images into
gray-scale images by using the green channel of the images. Our reasoning for
using gray-scale images was to enhance the important features while minimizing
any distracting nature of colors as gray-scale images are consistent across
many platforms and operating systems [36]. Also, we used the green channel as
the retina has a high sensitivity to this wavelength, thus this would yield
optimal contrast visually with vascular structures. In addition, we also used
contrast-limited adaptive histogram equalization (CLAHE) to improve the
local-contrast of pixels for more clear definition of features, which is
essential for interpreting the images as accurately as possible. The images
following pre-processing, including five classes, are shown in Figure 2.
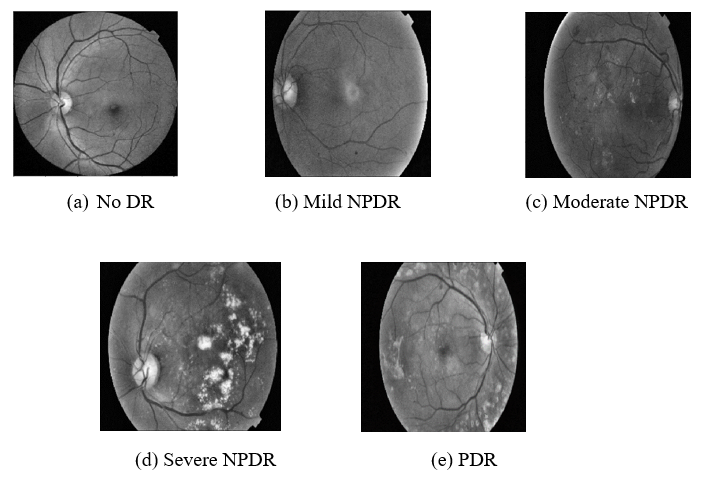
Figure 2: Examples of preprocessed images at various stages
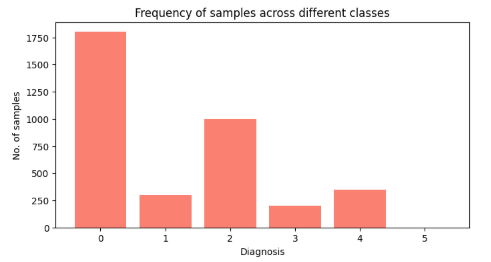
Figure 3: Imbalanced class distribution in Aptos-19 dataset.
We considered
the unbalanced class distributions found in the aptos-19 dataset, shown in
Figure 3, we used data augmentations to resolve this issue and improve the performance
of our proposed method. We adopted basic types of augmentations such as
rotation, horizontal flips, vertical flips, and mirroring to produce a balanced
dataset, as we wanted to amplify learning from a balanced training dataset. We
employed augmentations to provide a more performant computational approach and
additionally encouraged a more comprehensive view of diabetic retinopathy (DR)
by providing a more diverse or diverse and representative training dataset.
The primary
objective of our research is to develop a robust and high-performing
architecture capable of accurately identifying and categorizing diabetic
retinopathy (DR) from fundus images. To harness the potential of deep
pre-trained neural networks, we propose leveraging pre-trained ResNetV2[14] and
MobileNet[15] models to extract intricate features from fundus images. We will
facilitate two separate capsule networks with these extracted features so that
more intricate spatial representations could be achieved. By utilizing
pre-trained networks, we aim to maximize the extraction of fine features from
the images while minimizing the computational burden associated with training
from scratch. We hypothesize that features extracted from the Convolutional
base will encapsulate crucial fundus characteristics, thus facilitating
effective DR detection. In order to make it work; we keep the other layers
frozen and remove the layers that are near the output layers. Consequently, the
convolution base used to derive the fundus’s spatial properties is the
frozen layers.
In
contrast to conventional Convolutional neural network (CNN) architectures[48],
our proposed methodology integrates capsule layers to extract lower-level
information from feature maps generated by the pre-trained ResNet and MobileNet
architectures. Unlike CNNs, capsule networks exhibit resistance to rotation and
transformation while preserving spatial information across the network. Central
to capsule networks is the concept of capsules, comprising neurons that
determine the likelihood and direction of specific elements in an image
[16][17].
In
this framework, every capsule encapsulates the outcome as a condensed vector of
rich information following a series of complex operations applied to the input.
These operations include affine transformation, weighted summation, and
squashing, as detailed in equations (1-3).
Let's denote
 as the output
vector at the higher-level capsule j in layer
l+1, and p represents the input vector from a lower-level capsule i in layer l.
Through affine transformation, the lower-level features undergo encoding into a
higher-level abstract representation, facilitating the information transfer and
abstraction process[47].The lower-level features are encoded into a
higher-level abstract representation using the affine transformation
as described below:
as the output
vector at the higher-level capsule j in layer
l+1, and p represents the input vector from a lower-level capsule i in layer l.
Through affine transformation, the lower-level features undergo encoding into a
higher-level abstract representation, facilitating the information transfer and
abstraction process[47].The lower-level features are encoded into a
higher-level abstract representation using the affine transformation
as described below:
|

|
(1)
|
Here,
 denotes the
weight matrix responsible for learning to associate input features during the
model's learning phase. Subsequently, a weighted summation operation is
conducted to calculate the output of capsule j at layer l+1.
denotes the
weight matrix responsible for learning to associate input features during the
model's learning phase. Subsequently, a weighted summation operation is
conducted to calculate the output of capsule j at layer l+1.
|
|
(2)
|
In this context,
 represents the
coupling coefficients, satisfying the condition
represents the
coupling coefficients, satisfying the condition
 =1 and
=1 and
 for all j.
These coefficients are derived through the dynamic routing algorithm. Subsequently,
a squash function is applied, comprising a scaling term followed by a
normalization term.
for all j.
These coefficients are derived through the dynamic routing algorithm. Subsequently,
a squash function is applied, comprising a scaling term followed by a
normalization term.
|
|
(3)
|
The
model we propose employs a series of non-linear layers to capture spatial
representations and DR-specific details. The initial non-linearity stems from
deep pre-trained convolutional models, followed by another layer of
non-linearity introduced by capsule layers. The mathematical expressions for
this concept can be articulated as follows:
Let
 denote the
function representing the deep pre-trained convolutional models, where
x represents the input data. Similarly, let
denote the
function representing the deep pre-trained convolutional models, where
x represents the input data. Similarly, let
 represent the
function associated with the capsule layers. Thus, the overall model's output can
be expressed as:
represent the
function associated with the capsule layers. Thus, the overall model's output can
be expressed as:
|

|
(4)
|
This
formulation encapsulates the sequential application of non-linear layers in
capturing spatial representations and DR-specific details.
Once
more, we utilize capsule networks to create an ensemble learning
model. As we already know, ensemble
models surpass single models in terms of performance;
therefore, it is believed that the suggested
ensemble capsule network will benefit from both separate capsule
networks and contribute to improving overall model performance[45][46].
In
our plan, we have two capsule networks: one connected to the ResNet model's convolution
basis and the other to Mobile Net’sconvolution base. A softmax layer connects
each capsule network to generate the likelihood of the different classes. Let
us take
 ,
which are the scores generated by thei-th
capsule's softmax layer. We use a fully connected neural network model to
create this stochastic ensemble technique, and the computation can be expressed
as:
,
which are the scores generated by thei-th
capsule's softmax layer. We use a fully connected neural network model to
create this stochastic ensemble technique, and the computation can be expressed
as:
|

|
(5)
|
|
|
(6)
|
We
expect the model to dynamically adjust the weights for combining the output
scores of the capsule networks through the use of a stochastic ensemble. This
approach is anticipated to enhance DR detection and categorization
capabilities.
Finally,
we illustrate the overall framework of the proposed methodology in Figure 4.The
diagram depicts a sophisticated ensemble capsule network architecture proposed
for diabetic retinopathy classification from fundus images. The algorithm
starts with raw retina fundus images, which are initially processed through a
preprocessing phase. Preprocessing includes resizing the images, conversion
into grayscale by extracting the green channel, and enhancement of contrast
through algorithms like CLAHE. These operations are essential to increase the
prominence of relevant features and for providing uniformity to the input
images prior to their ingestion into the neural networks.
Following
preprocessing, the images are both passed through two independent convolutional
neural network (CNN) backbones, specifically ResNetV2 and MobileNet. Both CNNs
serve as feature extractors, generating rich and hierarchical representations
of the retinal images. It is common for these CNN convolutional layers to be
frozen at training to preserve their learned weights and lower computational
cost. The ResNetV2 output is depicted by green feature maps, whereas the MobileNet
output is represented by purple feature maps. The feature maps extracted by
both CNN backbones are reshaped afterward into a form that can be used for
capsule network input. Reshaping reduces the high-dimensional spatial feature
maps to tensors that can be understood by capsule layers, allowing for the
representation of spatial hierarchies in the data.
After
reshaping, the feature maps undergo processing by capsule network layers. Each
backbone's reorganized features first pass through a Primary Capsule layer,
where capsules of neurons encode not just the presence but also the pose and
spatial relationships of the identified features. The Class Capsule layer then
pools these capsules to represent particular diabetic retinopathy classes.
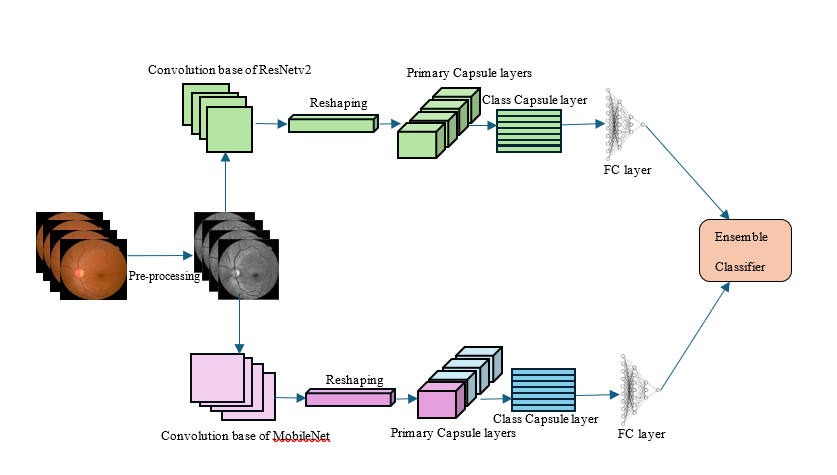
Figure 4. Block
diagram of the proposed methodology.
Capsule
networks are especially effective in medical images since they preserve spatial
hierarchies and are insensitive to rotations and deformations of images, which
are typical issues in retinal scans. These outputs from the capsule layers are
then sent through fully connected (FC) layers that convert the capsule outputs
to class scores or probabilities for a particular diabetic retinopathy
category. Basically, these FC layers serve as classifiers that approximate how
likely every DR stage is. Lastly, the model uses an ensemble classifier that
combines the outputs of both FC layers—one linked to the ResNetV2 capsule
network and the other linked to the MobileNet capsule network. Through this
combination of predictions, the ensemble takes advantage of the complementary strengths
of both CNN backbones and capsule representations to yield better
classification accuracy and resilience. This combination can be performed
through weighted averaging or trainable mechanisms. In short, this design
combines the strong feature extraction performance of pretrained CNNs and the
spatial cognition and stability of capsule networks in an ensemble approach.
Such a composite method seeks to improve automated diabetic retinopathy
detection and classification in fundus images through capturing multiple and
complementary feature representations.
The pseudocode
algorithm shown below provides a clear and structured representation of the
methodology used in the approach for automating diabetic retinopathy diagnosis
and classification.
Algorithm: Deep LearningEnsemble Methodology for Fundus Image Classification
1. Data Preprocessing:
Step 1.1: Load fundus images from the dataset.
Step 1.2: For each image:
a. Apply CLAHE to enhance image contrast:
b. Extract the green channel from the enhanced image.
c. Resize the image to 224x224 pixels
2. Data Augmentation:
Step 2.1: Initialize Image Data Generator with augmentation techniques (rotation, shift, flip, shear, zoom, fill mode).
Step 2.2: Generate augmented images in batches using `flow` method.
3. Feature Extraction using Pre-trained Models:
Step 3.1: Load pre-trained ResNetV2 and MobileNet models without their top layers.
Step 3.2: For each pre-trained model:
a. Freeze the layers to retain learned features.
b. Extract deep features from the training images.
c. Reshape the extracted features.
4. Capsule Network Implementation:
Step 4.1: Define a custom Capsule Network architecture with dense layers.
Step 4.2: For each pre-trained model's extracted features:
a. Compile the Capsule Network with Adam optimizer and categorical cross-entropy loss.
b. Fit the Capsule Network to the extracted features and labels.
5. Ensemble Technique:
Step 5.1: Make predictions using the trained Capsule Networks.
Step 5.2: Combine predictions using an ensemble technique:
6. Evaluation:
Step 6.1: Compute evaluation metrics for the ensemble model:
a. Calculate Accuracy,precision,Recall,F1-score
Step 6.2: Plot ROC curve for multiclass predictions,Confusion matrix and accuracy curves
We
conducted all experiments for DR detection and classification using Python with
the PyTorch and Keas libraries. By closely observing the effectiveness of our
proposed approach and adjusting parameters within predefined limits, we
established optimal hyper parameters for all models. Specifically, we set the
learning rate to 0.0001, while the regularization rates for weights and biases
ranged from 0.001 to 0.1. To enhance training efficiency, we employed the ADAM
optimizer. We employed the Aptos 2019 blindness detection dataset, publicly
accessible via Kaggle [18]. This dataset contains 3,662 labeled images in the
training folder and 1,928 unlabeled images in the testing folder. Our
experimentation exclusively focused on labeled images. The dataset underwent a
partition into a 70:30 ratio for training and testing sets, respectively.
Augmentations were applied solely to the training set, maintaining the integrity
of the testing split.
Evaluation
of our ensemble capsule model's performance was based on accuracy, precision,
recall, and F-measure. These metrics were computed using equations (7)-(10),
where TP, FP, TN, and FN denote true positive, false positive, true negative,
and false negative, respectively.
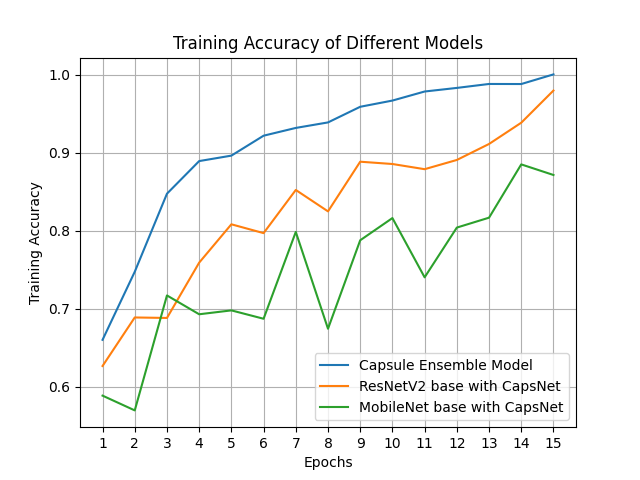
We
have depicted a visualization showcasing the performance of three different
models: a capsule network with ResNetV2, a capsule network with MobileNet, and
our proposed ensemble capsule network, as illustrated in Fig. 5. Notably, the
individual models exhibit commendable accuracy, which could be attributed to
the inherent capability of capsule networks to capture hierarchical
relationships among features, thereby offering a complementary representation
to that learned by traditional convolutional neural networks (CNNs) such as
ResNetV2 and MobileNet. Moreover, the introduction of ensemble learning leads
to a noticeable enhancement in performance. This improvement can be attributed
to the ability of the ensemble model to amalgamate predictions from multiple
models, thereby mitigating overfitting and achieving a more generalized
understanding of the data distribution.
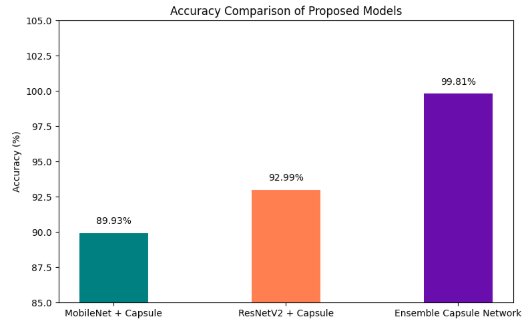
Figure 5. Comparison graph of different models.
We
have provided a detailed summary of the results in Table 3, presenting the
performance metrics of the proposed ensemble model alongside the two standalone
models that were combined.
Table 3. Performance of different proposed methodology.
|
Model
|
Accuracy
|
Precision
|
Recall
|
F-measure
|
|
MobileNet
Base with CapsuleNetwork
|
89.93
|
82.53
|
89.40
|
85.51
|
|
ResNetv2
Base with CapsuleNetwork
|
92.99
|
87.06
|
92.05
|
89.28
|
|
Ensemble
Capsule Network
|
99.81
|
99.89
|
99.40
|
99.64
|
We
performed an extensive hyperparameter tuning study to understand how various
parameters affect the performance of our ensemble capsule network for diabetic
retinopathy classification. The experiments focused on optimizing learning
rate, weight decay, batch size, dropout rate in capsule layers, routing
iterations, and ensemble weighting of backbone outputs.
Table 4
encapsulates the effect of learning rate, weight decay, and batch size. The
learning rate of 0.0001 always yielded the optimal results, with the highest
accuracy at 99.81%, along with better precision, recall, and F1-score. This
rate allowed for stable and smooth convergence during training. Higher learning
rates (e.g., 0.001) yielded oscillating loss and worse accuracy
(~93.42%).Values for weight decay (regularization) were essential in preventing
underfitting and overfitting. A moderate rate of 0.001 avoided overfitting without
compromising the model's capacity to learn complex retinal features. High
regularization (0.1) resulted in underfitting with decreased accuracy. The
batch size of 32 was an optimal choice between noisy gradients and stable
updates, enhancing the rate of convergence and generalization. Low batches (16)
caused slow convergence while high batches (64) diminished stochasticity,
negatively impacting generalization.
Table 4. Effect of Learning Rate, Weight Decay, and Batch Size on Model Performance
|
Learning Rate
|
Weight Decay
|
Batch Size
|
Accuracy (%)
|
Precision (%)
|
Recall (%)
|
F1-Score (%)
|
|
0.001
|
0.001
|
16
|
93.42
|
92.85
|
93.20
|
93.02
|
|
0.0005
|
0.01
|
32
|
96.88
|
96.50
|
96.70
|
96.60
|
|
0.0001
|
0.001
|
32
|
99.81
|
99.89
|
99.40
|
99.64
|
|
0.0001
|
0.1
|
64
|
98.12
|
97.80
|
97.50
|
97.65
|
Table
5 indicates the effect of dropout rate, routing iterations in capsule layers,
and ensemble weighting. A dropout rate of 0.3 in the capsule layers was able to
regularize the model without compromising learning capacity. Lower dropout
resulted in minor overfitting, whereas higher dropout (0.5) resulted in reduced
performance. Having 3 routing iterations within capsule layers enabled improved
feature agreement and information flow, improving model accuracy. Additional
iterations provided decreasing returns but higher computational expense. Ensemble
weighting benefited the ResNetV2 backbone with 60%, supporting the MobileNet
backbone's 40%, maximizing accuracy and stable classification performance.
MobileNet-favored or balanced weightings produced slightly less accurate
performance. Together, these results show why these hyperparameters need to be
carefully tuned. A combination of the capsule network with deep convolutional
feature extractors is significantly sensitive to the dynamics of an optimizer
and regularization. The adopted optimal values maximize this model's ability to
capture complex features and generalize well on diabetic retinopathy datasets.
Table 5: Effect of Dropout Rate, Routing Iterations, and Ensemble Weighting on Model Performance
|
Dropout Rate
|
Routing Iterations
|
Ensemble
Weighting (ResNetV2 / MobileNet)
|
Accuracy (%)
|
Precision (%)
|
Recall (%)
|
F1-Score (%)
|
|
0.1
|
1
|
0.4 / 0.6
|
93.42
|
92.85
|
93.20
|
93.02
|
|
0.3
|
3
|
0.5 / 0.5
|
96.88
|
96.50
|
96.70
|
96.60
|
|
0.3
|
3
|
0.6 / 0.4
|
99.81
|
99.89
|
99.40
|
99.64
|
|
0.5
|
5
|
0.7 / 0.3
|
98.12
|
97.80
|
97.50
|
97.65
|
To
evaluate the impact of individual architectural components on the
classification performance, we conducted an ablation study with six different
model configurations. These configurations include standalone CNN backbones,
capsule-only networks, combinations of CNNs with capsule layers, and the final
ensemble integrating both capsule-enhanced CNN models. Table 6 summarizes the
results across multiple metrics accuracy, precision, recall, and F1-score while
Figure 6 visually compares their performance.
Table 6: Performance
comparison of Different models
|
Model Variant
|
Accuracy (%)
|
Precision (%)
|
Recall (%)
|
F1-score (%)
|
|
ResNetV2
only
|
96.12
|
95.84
|
95.67
|
95.75
|
|
MobileNet
only
|
94.88
|
94.50
|
94.12
|
94.31
|
|
Capsule
only
|
92.45
|
91.83
|
91.56
|
91.69
|
|
ResNetV2
+ Capsule
|
98.34
|
98.20
|
98.10
|
98.15
|
|
MobileNet
+ Capsule
|
97.85
|
97.63
|
97.50
|
97.56
|
|
Proposed
Ensemble (ResNetV2 + MobileNet + Capsule)
|
99.81
|
99.85
|
99.79
|
99.82
|
Table
6 gives the quantitative comparison of performance between six model configurations
employed in our ablation study. ResNetV2 and MobileNet standalone CNN backbones
recorded decent accuracy rates of 96.12% and 94.88%, respectively, as seen in
their ability to extract useful features from OCTA images. The Capsule-only
model with no CNN-based feature extraction recorded the lowest accuracy
(92.45%), highlighting that capsule networks are not good enough for this
purpose without supporting deep feature representations. Combining capsule
layers with the CNN backbones dramatically improved performance; ResNetV2 +
Capsule and MobileNet + Capsule models enhanced accuracy by about 2.2% and 3%,
respectively, over their CNN-only counterparts. These improvements reflect the
robustness of the capsule layers in representing spatial hierarchies and
relationships essential for classifying diabetic retinopathy lesions. The
ensemble, which combines predictions of both capsule-augmented CNNs, further
raised performance to an impressive 99.81% accuracy, showing that it is
beneficial to combine different architectures to extract complementary features
and enhance robustness. Precision, recall, and F1-score measures also follow
similar patterns, supporting the ensemble's better balance between sensitivity
and specificity.
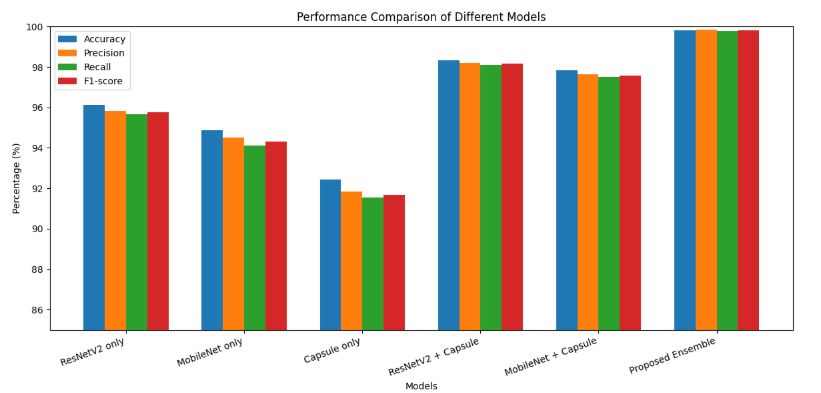
Figure 6: Performance comparison of Different models
The
interpretability of deep learning models is essential in clinical applications,
particularly in ophthalmology, where diagnostic confidence is tied not only to
accuracy but also to the transparency of decision-making. This study evaluates
interpretability through confusion matrices, ROC curve analysis, training
dynamics, and an examination of the capsule network’s inherent capability for
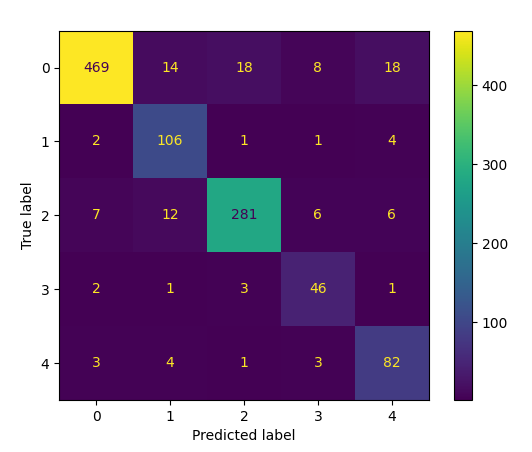
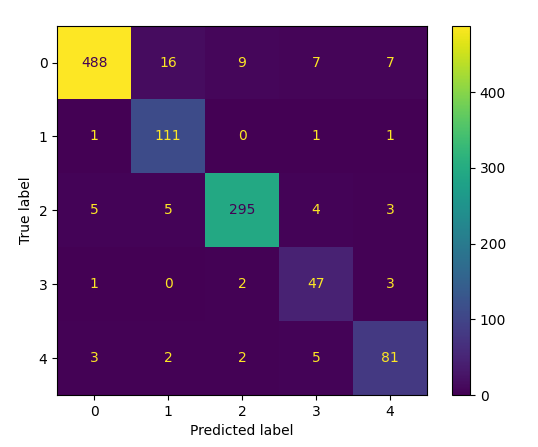
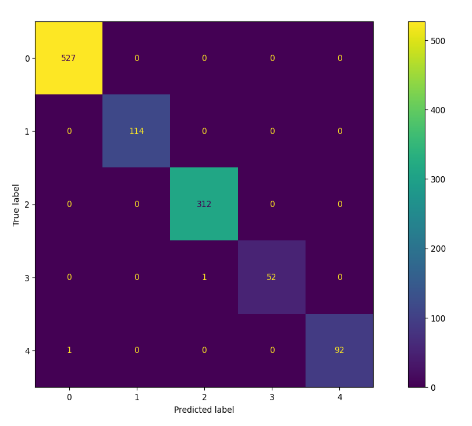
spatial feature preservation. Additionally, we have included the confusion
matrices obtained by these models in Fig. 7.
Figure 7: Confusion matrix obtained for (a) MobileNet Base
with Capsule Network, (b) ResNetV2 with Capsule Network, and (c) Ensemble
Capsule Network.
The
confusion matrices reveal clear differences in classification behavior between
the models. In the MobileNet+ Capsule configuration, misclassifications were
predominantly observed between mild and moderate DR classes. This is expected given the
subtle textural and vascular changes differentiating these categories. The
ResNetV2 + Capsule model showed a reduction in such errors, although mild
confusion persisted between severe and proliferative DR stages, where overlapping
pathological indicators can mislead the network. The ensemble model, however,
demonstrated minimal off-diagonal activity, signifying robust classification
boundaries across all five severity levels. Notably, its capacity to resolve
borderline cases particularly moderate versus severe DR addresses a critical
clinical challenge, as these distinctions often dictate whether invasive
treatment is warranted.
The
ROC analysis further substantiates the performance advantage of the ensemble
approach. The MobileNet + Capsule network achieved an average AUC of
approximately 0.95, while the ResNetV2 + Capsule reached around 0.97. In
contrast, the ensemble attained near-perfect separability with an AUC
approaching 0.999 across all classes. This marked improvement reflects the
synergy of feature diversity and decision stability achieved by integrating
multiple capsule-based CNN backbones, effectively balancing sensitivity and
specificity across the severity spectrum.
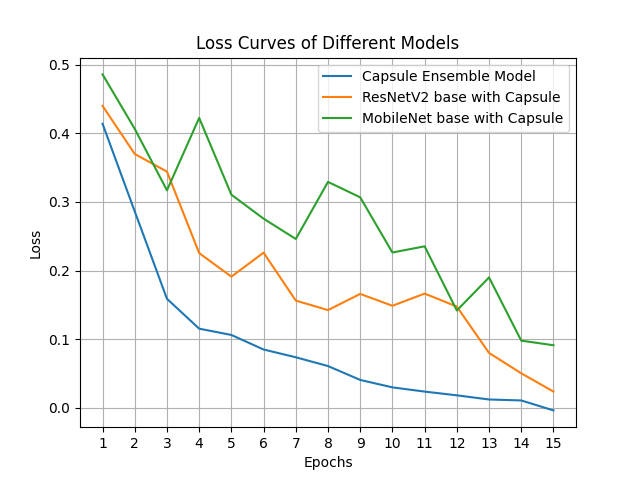
Furthermore, the ROC
curves of the three models are depicted in Figure. 8, while the accuracy and
loss curves are presented in Figure. 9.
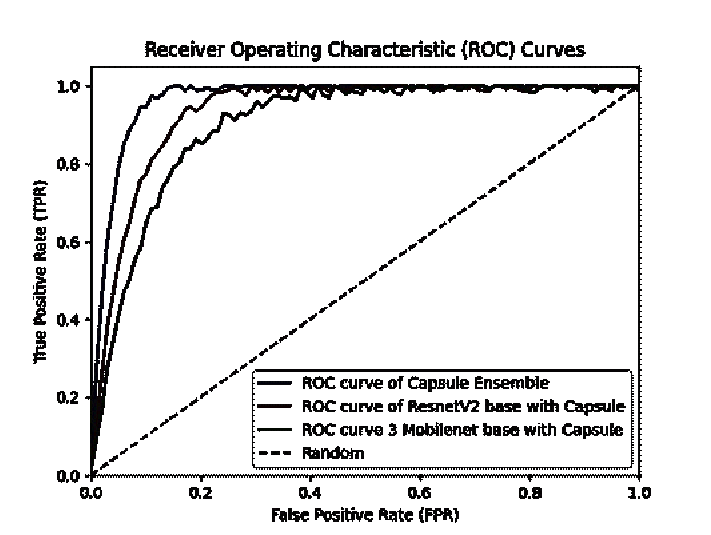
Figure 8. ROC of different models discussed.
The
training accuracy and loss plots for the ensemble model show rapid convergence
with stable validation performance, indicating that the chosen regularization
strategies, augmentation pipeline, and hyperparameter tuning effectively
mitigated overfitting. The smooth validation loss trajectory confirms that the
model maintained generalization capability despite achieving high training
accuracy, which is critical for deployment in real-world screening environments
with unseen data distributions.
Figure 9. Accuracy and Loss Curves of the discussed models
Our
model not only excels in classification metrics but also strengthens the domain
of scientific visualization and visual analytics. Through confusion matrices,
ROC curves, and class activation visualizations, we offer clinicians
interpretable insights into model behavior. The capsule layers further allow
visualization of hierarchical spatial relationships, enabling interpretability
of DR lesion detection across varying severity levels. These tools can support
ophthalmologists in understanding and validating automated decisions, thereby
bridging the gap between AI systems and clinical trust.
Although
class activation maps like Grad-CAM are not included in this study, our
proposed architecture contributes to scientific visualization and visual
analytics through multiple mechanisms. First, capsule networks inherently
preserve spatial hierarchies and pose information, enabling a more
interpretable feature representation compared to traditional CNNs. Second, we
provide extensive performance visualizations including confusion matrices, ROC
curves, and learning curves that help analyze model behavior in detail. These
visual outputs offer clinicians a meaningful understanding of the
classification patterns and potential misclassifications across DR severity
levels.
To
evaluate the performance of the suggested Stochastic Capsule Fusion Network, it
was compared with some of the latest state-of-the-art diabetic retinopathy
classification algorithms published in the literature. Table X provides a
listing of the models, techniques, and their respective classification
accuracies. The mentioned studies cover a range of deep learning models, from
simple CNN architectures like VGG-16, DenseNet201, Inception-v3, and
Inception-ResNet-v2 to complex hybrid designs like Hybrid Residual U-Net, Local
Binary CNN (LB-CNN), and multi-model ensembles of architectures like
DenseNet-121, Xception, Inception-v3, and ResNet-50.
These
methods have reported accuracies of between 84.6% for MSA-Net and 97.41% for
LB-CNN, and as such, there is significant variance in performance based on
architecture complexity, feature extraction approach, and dataset. Although
high performances are seen with models such as Inception-ResNet-v2 (97.0%) and
VGG-16 (96.86%), these methods essentially use convolutional layers to
represent features and do not have direct mechanisms to extract spatial
hierarchies and part–whole relationships. Conversely, the Stochastic Capsule
Fusion Network proposed in the paper attained a classification accuracy of
99.81%, surpassing every method compared. The performance boost can be ascribed
to the synergy of stochastic ensemble learning and capsule network layers that
improve robustness, maintain spatial relationships, and boost generalization.
The experiments illustrate that blending capsule-based feature modeling into an
ensemble scheme can serve to greatly improve the state of art for automatic
diabetic retinopathy detection. Moreover, a comparative analysis of our proposed
system against existing research models that utilized the Aptos-19 database has
been conducted, and the results are summarized in Table 7.
Table 7. Performance Comparison in terms of accuracy with existing models- APTOS Datasets.
|
Reference
|
Methodology
|
Accuracy
|
|
Al-Antary, M. T.
(2021)[27]
|
MSA-Net
|
84.6%
|
|
Oulhadj, M., et al.
(2022) [28]
|
Densenet-121, Xception,
Inception-v3, Resnet-50
|
85.28%
|
|
Crane, A., &
Dastjerdi, M. (2022) [29]
|
Inception-ResNet-v2
|
97.0%,
|
|
Escorcia-Gutierrez, J.,
et al. (2022) [30]
|
VGG-16
|
96.86%
|
|
Salluri, D. Ket al.. (2022)[31]
|
Hybrid Residual U-Net
|
94%
|
|
Kobat, S. G., et al.
(2022) [32]
|
DenseNet201
|
93.85%
|
|
Macsik, P., et al.
(2022) [33]
|
Local
binary-convolutional neural network (LB-CNN)
|
97.41%
|
|
Yadav, S., & Awasthi,
P. (2022 [34]
|
Inception-v3
|
88.1%
|
|
Proposed
Model
|
Stochastic
Capsule Fusion Network
|
99.81%
|
Our proposed
model for diabetic retinopathy diagnosis and classification significantly
outperforms existing models on the APTOS dataset. Our model achieved an
accuracy of 99.81%, compared to the best preceding accuracy of 94.20% from
Sikder et al. (2021) who also used tuned XGBoost. We also exceeded the
precision of Yongjia Lei's GF-CapsNet (2024) at 95.59% with a precision of
99.89%, and our recall of 99.40% is more than double from the previous best of
92.68% from Sikder et al. Furthermore, our model also achieved a F1-score of
99.64%, suggesting balanced expecation for all metrics but also indicating
sufficiently higher performance for one or more metrics. Through the
application of ensemble learning and a capsule network model, the ability to
capture finer spatial representations was beneficial for highly accurate DR
severity classifications. Combination of multiple deep learning models provide
more robust and reliable diagnostic output which also confirms that it is
suitable for clinical practice. The superior performance of the proposed model
verifies that diagnostic accuracy and reliability will improve, enhancing the
use of deep learning in DR diagnosis and management. A comparison of our
proposed system's performance related to existing research models that utilized
the Aptos-19 database was also completed, and is summarized in Table 8.
Table 8. Comparison of performance with existing models on APTOS 2019
|
Reference
|
Year
|
Methods
|
Accuracy (%)
|
Precision (%)
|
Recall (%)
|
F1-Score (%)
|
|
Sikder et al.[38]
|
2021
|
Tuned XGBoost
|
94.20
|
94.34
|
92.68
|
93.51
|
|
Islam et al.[39]
|
2022
|
SCL(Supervised contrastive
learning)
|
84.35
|
73.84
|
70.51
|
70.49
|
|
Oulhadj et al.[40]
|
2022
|
Ensemble
|
85.28
|
80.00
|
70.00
|
73.00
|
|
Bodapati et al.[41]
|
2022
|
Stacked Convolutional
Auto Encoder(SCAE)
|
86.08
|
76.00
|
82.00
|
-
|
|
Oulhadj et al.[42]
|
2023
|
Ensemble(CapsNet+
Inception Block+Discrete
Wavelet Transform)
|
86.54
|
76.00
|
70.00
|
73.00
|
|
Mondal et al.[43]
|
2023
|
Ensemble Method
|
86.08
|
76.00
|
82.00
|
-
|
|
Yongjia Lei[44]
|
2024
|
Graph Neural Network (GNN)-fused CapsNet
|
86.49
|
0.9559
|
0.7914
|
0.7101
|
|
Proposed
Model
|
2024
|
Ensemble
Capsule Network
|
99.81
|
99.89
|
99.40
|
99.64
|
The
increasing incidence of diabetes-related complications, especially diabetic
retinopathy (DR), is a serious problem worldwide and diabetic retinopathy is
the most important cause of vision impairment across the globe. The grading and
detection of DR lesions by ophthalmologists manually are an arduous and
time-consuming process. This study aimed to tackle this issue by utilizing
advances in deep learning methods to create an automated DR diagnosis and
classification system. By combining a number of pre-trained deep learning
networks layers with capsule network layers for feature extraction and
employing a stochastic ensemble process for classification with fundus images,
our proposed solution provides an opportunity to assist ophthalmologists with
accurate diagnoses and grading of DR. Evaluation of the proposed model using
the Aptos-19 dataset showed stellar results, with an overall testing accuracy
of 99.81%. The accuracy highlights the potential of the method for improving
both the efficiency and effectiveness of DR diagnosis and grading. Future work
could explore if integration with an interactive visual analytics dashboards,
enabling dynamic searching and exploration of DR diagnosis, lesion heatmaps,
and class-specific prediction trajectories, would provide transparency and
decision support and encourage clinical implementation. Further research and
validation on diverse datasets and real-world clinical settings will be
essential to confirm the generalizability and robustness of the proposed
methodology. Additionally, efforts to streamline the integration of automated
DR diagnosis systems into clinical practice and healthcare workflows are
warranted to ensure widespread adoption and impact.
The
authors declare that we have no conflict of interest. On behalf of all authors, the corresponding author states
that there is no conflict of interest.
APTOS
2019 datasets are freely available to the public and were contributed by
Kaggle, which the authors thank for this
1. Kropp, M., Golubnitschaja, O., Mazurakova, A., Koklesova, L., Sargheini, N., Vo, T. K. S., de Clerck, E., Polivka, J., Jr, Potuznik, P., Polivka, J., Stetkarova, I., Kubatka, P., &Thumann, G. (2023). Diabetic retinopathy as the leading cause of blindness and early predictor of cascading complications—Risks and mitigation. The EPMA Journal, 14(1), 21–42. https://doi.org/10.1007/s13167-023-00314-8
2. Shin, E. S., Sorenson, C. M., & Sheibani, N. (2014). Diabetes and retinal vascular dysfunction. Journal of Ophthalmic and Vision Research, 9(3), 362–373. https://doi.org/10.4103/2008-322X.143378
3. Gargeya R., Leng T. Automated Identification of Diabetic Retinopathy Using Deep Learning. Ophthalmology. 2017;124:962–969. doi: 10.1016/j.ophtha.2017.02.008.
4. International Diabetes Federation. (2022, November 24). Facts & figures. https://idf.org/about-diabetes/diabetes-facts-figures/
5. Press Information Bureau. (2025, July 20). Update on treatment of diabetes. https://pib.gov.in/PressReleasePage.aspx?PRID=1944600
6. Alyoubi, W. L., Shalash, W. M., & Abulkhair, M. F. (2020). Diabetic retinopathy detection through deep learning techniques: A review. Informatics in Medicine Unlocked, 20, 100377. https://doi.org/10.1016/j.imu.2020.100377
7. Tymchenko, B., Marchenko, P., & Spodarets, D. (2020). Deep learning approach to diabetic retinopathy detection [Preprint]. arXiv. https://arxiv.org/abs/2003.11544
8. Gangwar, A. K., & Ravi, V. (2021). Diabetic retinopathy detection using transfer learning and deep learning. In V. Bhateja, S. L. Peng, S. C. Satapathy, & Y. D. Zhang (Eds.), Evolution in computational intelligence (Vol. 1176). Springer. https://doi.org/10.1007/978-981-15-5788-0_64
9. Karki, S. S., & Kulkarni, P. (2021). Diabetic retinopathy classification using a combination of EfficientNets. In 2021 International Conference on Emerging Smart Computing and Informatics (ESCI) (pp. 68–72). IEEE. https://doi.org/10.1109/ESCI50559.2021.9397035
10. Mishra, S., Hanchate, S., & Saquib, Z. (2020). Diabetic retinopathy detection using deep learning. In 2020 International Conference on Smart Technologies in Computing, Electrical and Electronics (ICSTCEE) (pp. 515–520). IEEE. https://doi.org/10.1109/ICSTCEE49637.2020.9277506
11. A., A. M., & Priya, S. S. S. (2025). A novel deep learning approach for diabetic retinopathy classification using optical coherence tomography angiography. Multimedia Tools and Applications. Advance online publication. https://doi.org/10.1007/s11042-025-20708-2
12. Abini, M. A., & Sridevi Sathya Priya, S. (2025). Detection and classification of diabetic retinopathy using modified Inception V3. International Journal Bioautomation, 29(1), 77–92. https://doi.org/10.7546/ijba.2025.29.1.001004
13. A., M. A., & Sathya Priya, S. S. (2025). A survey on computer aided systems for diabetic retinopathy detection and classification using deep learning. In 2025 International Conference on Electronics and Renewable Systems (ICEARS) (pp. 1475–1480). IEEE. https://doi.org/10.1109/ICEARS64219.2025.10940665
14. A., M. A., & Sathya Priya, S. S. (2023). A deep learning framework for detection and classification of diabetic retinopathy in fundus images using residual neural networks. In 2023 9th International Conference on Smart Computing and Communications (ICSCC) (pp. 55–60). IEEE. https://doi.org/10.1109/ICSCC59169.2023.10335079
15. Mushtaq, G., & Siddiqui, F. (2021). Detection of diabetic retinopathy using deep learning methodology. IOP Conference Series: Materials Science and Engineering, 1070(1), 012049. https://doi.org/10.1088/1757-899X/1070/1/012049
16. AbdelMaksoud, E., Barakat, S., & Elmogy, M. (2022). A computer-aided diagnosis system for detecting various diabetic retinopathy grades based on a hybrid deep learning technique. Medical & Biological Engineering & Computing, 60, 2015–2038. https://doi.org/10.1007/s11517-022-02564-6
17. Chowdhury, P., Islam, M. R., Based, M. A., & Chowdhury, P. (2021). Transfer learning approach for diabetic retinopathy detection using efficient network with 2 phase training. In 2021 6th International Conference for Convergence in Technology (I2CT) (pp. 1–6). IEEE. https://doi.org/10.1109/I2CT51068.2021.9418111
18. A., M. A., & Sathya Priya, S. S. (2023). Detection and classification of diabetic retinopathy using pretrained deep neural networks. In 2023 International Conference on Innovations in Engineering and Technology (ICIET) (pp. 1–7). IEEE. https://doi.org/10.1109/ICIET57285.2023.10220715
19. Abini, M. A., & Priya, S. S. S. (2025). Advanced capsule networks for accurate detection and classification of diabetic retinopathy from fundus images. In S. Manoharan, A. Tugui, & I. Perikos (Eds.), Proceedings of 5th International Conference on Artificial Intelligence and Smart Energy (ICAIS 2025) (Information Systems Engineering and Management, vol. 41). Springer. https://doi.org/10.1007/978-3-031-90478-3_37
20. Abini, M. A., & Priya, S. S. S. (2025). Automatic detection and classification of diabetic retinopathy from optical coherence tomography angiography images using deep learning – A review. AIUB Journal of Science and Engineering, 23(3), 277–297.
21. A., M. A., Vinod, A., Rafeeque, S., Manju, T. S., & Noushad, M. S. (2024). MobileNet-enhanced skin cancer detection and classification using dermatoscopic images. In 2024 IEEE International Conference on Smart Power Control and Renewable Energy (ICSPCRE) (pp. 1–6). IEEE. https://doi.org/10.1109/ICSPCRE62303.2024.10674858
22. Khan, A., Chefranov, A., & Demirel, H. (2023). Building discriminative features of scene recognition using multi-stages of inception-ResNet-v2. Applied Intelligence, 53(15), 18431–18449. https://doi.org/10.1007/s10489-023-04460-4
23. Howard, A. G., Zhu, M., Chen, B., Kalenichenko, D., Wang, W., Weyand, T., Andreetto, M., & Adam, H. (2017). MobileNets: Efficient convolutional neural networks for mobile vision applications. arXiv:1704.04861. https://doi.org/10.48550/arXiv.1704.04861
24. Rangel, G., Cuevas-Tello, J. C., Rivera, M., & Renteria, O. (2023). A Deep Learning Model Based on Capsule Networks for COVID Diagnostics through X-ray Images. Diagnostics, 13(17), 2858. https://doi.org/10.3390/diagnostics13172858
25. M. A., A., & Sridevi Sathya Priya, S. (2025). Deep learning-based diabetic retinopathy classification of augmented fundus images using convolutional neural networks. International Journal of Image and Graphics, 25(03), 2750040. https://doi.org/10.1142/S0219467827500409
26. A. M., A., & Priya, S. S. S. (2025). Ensemble models for diabetic retinopathy detection and classification using vision transformers and capsule networks with advanced feature extraction techniques. Australian Journal of Electrical and Electronics Engineering, 1–22. https://doi.org/10.1080/1448837X.2025.2539557
27. Al-Antary, M. T., & Arafa, Y. (2021). Multi-scale attention network for diabetic retinopathy classification. IEEE Access, 9, 54190–54200. https://doi.org/10.1109/ACCESS.2021.3070685
28. Oulhadj, M., Riffi, J., Chaimae, K., El Hassani, A., & Merbouha, A. (2022). Diabetic retinopathy prediction based on deep learning and deformable registration. Multimedia Tools and Applications, 81, 28709–28727. https://doi.org/10.1007/s11042-022-12968-z
29. Crane, A. B., Choudhry, H. S., & Dastjerdi, M. H. (2024). Effect of simulated cataract on the accuracy of artificial intelligence in detecting diabetic retinopathy in color fundus photos. Indian Journal of Ophthalmology, 72(Suppl 1), S42–S45. https://doi.org/10.4103/IJO.IJO_1163_23
30. Escorcia-Gutierrez, J., et al. (2022). Analysis of pre-trained convolutional neural network models in diabetic retinopathy detection through retinal fundus images. In: Saeed, K., Dvorsky, J. (eds.) Computer Information Systems and Industrial Management. CISIM 2022. Lecture Notes in Computer Science, vol. 13293, pp. 167–178. Springer, Cham. https://doi.org/10.1007/978-3-031-10539-5_15
31. Salluri, D. K., Sistla, V., & Kolli, V. K. K. (2023). HRUNET: Hybrid residual U-Net for automatic severity prediction of diabetic retinopathy. Computer Methods in Biomechanics and Biomedical Engineering: Imaging & Visualization, 11(3), 530–541. https://doi.org/10.1080/21681163.2022.208302
32. Kobat, S. G., Baygin, N., Yusufoglu, E., Baygin, M., Barua, P. D., Dogan, S., Yaman, O., Celiker, U., Yildirim, H., Tan, R. S., Tuncer, T., Islam, N., & Acharya, U. R. (2022). Automated diabetic retinopathy detection using horizontal and vertical patch division-based pre-trained DenseNet with digital fundus images. Diagnostics, 12(8), 1975. https://doi.org/10.3390/diagnostics12081975
33. Macsik, P., Pavlovicova, J., Goga, J., & Kajan, S. (2022). Local binary CNN for diabetic retinopathy classification on fundus images. Acta Polytechnica Hungarica, 19(7), 27–45. https://doi.org/10.12700/APH.19.7.2022.7.2
34. Yadav, S., & Awasthi, P. (2022). Diabetic retinopathy detection using deep learning and Inception-V3 model. International Research Journal of Modern Engineering and Technology Science, 4, 1731–1735.
35. Canayaz, M. (2022). Classification of diabetic retinopathy with feature selection over deep features using nature-inspired wrapper methods. Applied Soft Computing, 128, 109462. https://doi.org/10.1016/j.asoc.2022.109462
36. Bodapati, J. D., Rohith, V. N., & Dondeti, V. (2022). Ensemble of deep capsule neural networks: An application to pediatric pneumonia prediction. Physical and Engineering Sciences in Medicine, 45(3), 949–959. https://doi.org/10.1007/s13246-022-01169-5
37. “APTOS 2019 blindness detection,” Kaggle.com. [Online]. Available: https://www.kaggle.com/c/aptos2019-blindness-detection/data. [Accessed: 2-July -2025].
38. Sikder, N., Masud, M., Bairagi, A. K., Arif, A. S. M., Nahid, A.-A., & Alhumyani, H. A. (2021). Severity classification of diabetic retinopathy using an ensemble learning algorithm through analyzing retinal images. Symmetry, 13(4), 670. https://doi.org/10.3390/sym13040670
39. Islam, M. R., Abdulrazak, L. F., Nahiduzzaman, M., Goni, M. O. F., Anower, M. S., Ahsan, M., Haider, J., & Kowalski, M. (2022). Applying supervised contrastive learning for the detection of diabetic retinopathy and its severity levels from fundus images. Computers in Biology and Medicine, 146, 105602. https://doi.org/10.1016/j.compbiomed.2022.105602
40. Oulhadj, M., Riffi, J., & Chaimae, K. (2022). Diabetic retinopathy prediction based on deep learning and deformable registration. Multimedia Tools and Applications, 81, 28709–28727. https://doi.org/10.1007/s11042-022-12659-8
41. Bodapati, J. D. (2022). Stacked convolutional auto-encoder representations with spatial attention for efficient diabetic retinopathy diagnosis. Multimedia Tools and Applications, 81, 32033–32056. https://doi.org/10.1007/s11042-022-12942-8
42. Oulhadj, M., Riffi, J., Khodriss, C., Mahraz, A. M., Bennis, A., Yahyaouy, A., Chraibi, F., Abdellaoui, M., Andaloussi, I. B., & Tairi, H. (2023). Diabetic retinopathy prediction based on wavelet decomposition and modified capsule network. Journal of Digital Imaging, 36(4), 1739–1751. https://doi.org/10.1007/s10278-023-00872-x
43. Mondal, S. S., Mandal, N., Singh, K. K., Singh, A., & Izonin, I. (2023). EDLDR: An ensemble deep learning technique for detection and classification of diabetic retinopathy. Diagnostics, 13(1), 124. https://doi.org/10.3390/diagnostics13010124
44. Lei, Y., Lin, S., Li, Z., Zhang, Y., & Lai, T. (2024). GNN-fused CapsNet with multi-head prediction for diabetic retinopathy grading. Engineering Applications of Artificial Intelligence, 133, 107994. https://doi.org/10.1016/j.engappai.2023.107994
45. Abini, M. A., & Sridevi Sathya Priya, S. (2025). Multistage classification of diabetic retinopathy in fundus images using hybrid capsule networks. Journal of Multiscale Modelling. https://doi.org/10.1142/S1756973725500064
46. Abini, M.A., Sridevi Sathya Priya, S. (2025). DRDResNet—A Deep Learning Model for Diabetic Retinopathy Detection and Classification. In: Kanhe, A., Balanethiram, S., Hsiung, PA., Jayakody, D.N.K. (eds) Advances in VLSI, Signal Processing and Wireless Communication. IEdTC 2023. Lecture Notes in Electrical Engineering, vol 1323. Springer, Singapore. https://doi.org/10.1007/978-981-96-1587-2_12
47. Abini, M.A., Priya, S.S.S. (2025). An Augmented Efficient Net Based Deep Learning Model for Diabetic Retinopathy Detection and Classification. In: Soni, B., Saini, P., Verma, G.K., Gupta, B.B. (eds) Beyond Artificial Intelligence. AICTA 2023. Lecture Notes in Networks and Systems, vol 1326. Springer, Singapore. https://doi.org/10.1007/978-981-96-4170-3_26
48. Naseer, R. K., Afzal, A., Arshaq, M., R. K. M., & A. M. A. (2025). RiViT – Rice leaf disease identification and classification using vision transformer (ViT). 2025 4th International Conference on Advances in Computing, Communication, Embedded and Secure Systems (ACCESS), 245–250. IEEE. https://doi.org/10.1109/ACCESS65134.2025.11135614